Yukineonroids
Newbie
- Thread Author
- #1
20 years old, Testosterone Enanthate, HCG, Clenbuterol
The great myth that Leydig cells have a habituation effect and are unnecessarily desensitized is wrong. The saying goes "the dose makes the poison" – as long as the dose is kept moderate and in a therapeutic dose such as 250IU 2 times per week, this does not necessarily lead to desensitization. In most cases these occur with higher dosages such as 2500IU per week with long-term use. Why it is important to know this is that with extreme high-dose use without HCG support, Leydig cell damage can occur which under certain circumstances can persist and thus represent a permanent state, which is why there is also the possibility that you have to permanently inject yourself with testosterone because your body can no longer produce it itself.
The disadvantages of clenbuterol are as follows: elevated heart rate and high adrenaline levels. Since clenbuterol indirectly promotes adrenaline release and thus also brings tremor and nervousness. In addition, there is the so-called type 2 fiber shift, where the endurance-oriented muscle fibers switch to fast-twitch muscle fibers with reduced endurance. Some see that as an advantage, some as a disadvantage. Then there are the cardiovascular risks, as your cardiovascular system can suffer damage. The beta 2 receptor desensitization: here it is so that with every day of clenbuterol use, the beta 2 receptors become saturated and thus after a while desensitize and thus clenbuterol can no longer produce positive effects, which is why you stick to the most famous scheme of 2 weeks on 2 weeks off so that the receptors can recover and are no longer desensitized.
Based on my blood test, you can see that my HDL/LDL value is extremely bad, which is due to the fact that I did not do any cardio training to stabilize these values. To do this now, I additionally do cardio, supplement more omega 3, and continue my diet for body fat reduction.
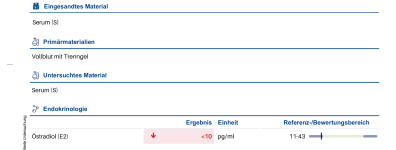
You can also see that my estradiol E2 value is extremely elevated, which is due to my high body fat percentage. As a countermeasure, I have decided to take an aromatase inhibitor. I personally decided on anastrozole 0.5mg daily (ED) and will therefore do another quick lab test for my estradiol in 7 days to see how quickly it drops and then in 14 days when steady state is reached, do another lab test for my estradiol to adjust the dosage accordingly.
Important: With E2 = 162 pg/ml, monitoring is particularly critical because my body fat is simultaneously decreasing (through diet + clen) and this also lowers aromatase activity. This means my E2 could drop faster than normal and therefore I should already check after 7 days to not overshoot.
For you as a nice to know: please consider that there are anastrozole non-responders and if you should be one of them, you should switch to other aromatase inhibitors such as exemestane or letrozole etc.
I wrote the complete text myself, but I had it translated into English by an AI since I'm not that good at writing in this language as I'm from Germany. I created the tables myself for a structured overview. I hope I don't get hate for this since I just want to help. Thank you all!
Starting Stats
- 20 years old
- 90 kg
- 167cm
- 35% BF
Current Stats (Week 6)
- 20 years old
- 94 kg
- 167cm
- 30% BF
Foreword
First of all, I want to thank Driadashop.to for providing me with this platform to share my knowledge with you. Most importantly, I want to say that all statements made here are without warranty.Why did I start taking AAS at 20 years old?
The reason for this is that there was no doctor who could help me solve my problems. I had a testosterone deficiency and every doctor wanted to prescribe me antidepressants for my symptoms, which I personally strongly opposed. After that, I really intensively engaged with this entire topic and did not even bother to look at bro science things, but instead immediately engaged deeply with the subject and only looked at validated scientific studies and analyzed them systematically.Why I chose Testosterone Enanthate, HCG, and Clenbuterol
Testosterone Enanthate (2x 125mg = 250mg per week)
Due to my hypogonadism, I chose testosterone enanthate because it is not a foreign substance to the body and should therefore be a baseline in every cycle and is also used in medical TRT in Germany. With this dosage, I reached over 13 ng/ml testosterone at trough in a blood test after 6 weeks, which shows that I am a very good responder.HCG (2x 250IU = 500IU per week)
I take HCG in a very low dosage which is minimal to prevent testicular atrophy and so that I can maintain the stimulation of my Leydig cells so that they do not shrink and later when I eventually stop there are no long-term damages. The mechanism of action of HCG is as follows: HCG imitates the body's own LH and works on these receptors which promote spermatogenesis and result in the maintenance of testicular capacity.The great myth that Leydig cells have a habituation effect and are unnecessarily desensitized is wrong. The saying goes "the dose makes the poison" – as long as the dose is kept moderate and in a therapeutic dose such as 250IU 2 times per week, this does not necessarily lead to desensitization. In most cases these occur with higher dosages such as 2500IU per week with long-term use. Why it is important to know this is that with extreme high-dose use without HCG support, Leydig cell damage can occur which under certain circumstances can persist and thus represent a permanent state, which is why there is also the possibility that you have to permanently inject yourself with testosterone because your body can no longer produce it itself.
Clenbuterol (120mcg daily in a 2 weeks on / 2 weeks off scheme)
I personally took clenbuterol because of my diet, as the drug can bring many advantages but also strong side effects. The advantage of clenbuterol is that it is a beta 2 agonist which increases thermogenesis and thus as a nice side effect brings an additional kcal expenditure of approximately 200-300kcal depending on the dosage. However, the great advantage of clenbuterol is that it mobilizes the fat depots and increases fat oxidation by approximately 30-40%, which results in your body not only drawing on muscles, glycogen and fat but drawing approximately 80-90% only on fat under optimal conditions such as macros, deficit, training. In addition, clenbuterol brings a muscle-sparing effect.The disadvantages of clenbuterol are as follows: elevated heart rate and high adrenaline levels. Since clenbuterol indirectly promotes adrenaline release and thus also brings tremor and nervousness. In addition, there is the so-called type 2 fiber shift, where the endurance-oriented muscle fibers switch to fast-twitch muscle fibers with reduced endurance. Some see that as an advantage, some as a disadvantage. Then there are the cardiovascular risks, as your cardiovascular system can suffer damage. The beta 2 receptor desensitization: here it is so that with every day of clenbuterol use, the beta 2 receptors become saturated and thus after a while desensitize and thus clenbuterol can no longer produce positive effects, which is why you stick to the most famous scheme of 2 weeks on 2 weeks off so that the receptors can recover and are no longer desensitized.
How did I start?
Before I started, I did a blood test to know my baseline values. Unfortunately, I had prepared very fatty food the evening before, which resulted in certain values in my blood test not being measurable or being falsified, which I regret afterwards because these values are really important.PEDs
| Testosterone Enanthate | 125mg | 2x per week |
| HCG | 250IU | 2x per week |
Training
| Monday | 6 sets chest / 4 sets triceps | 10 |
| Tuesday | 6 sets back / 4 sets biceps | 10 |
| Wednesday | Rest Day | — |
| Thursday | 6 sets biceps / 6 sets triceps / 6 sets shoulders | 18 |
| Friday | 4 sets chest / 4 sets back | 8 |
| Saturday | Rest Day | — |
| Sunday | Rest Day | — |
Why did I choose this training plan?
I chose this training plan because it is the most effective for me. I train really hard every set to muscle failure or just before muscle failure with steady weight increases. The reason I don't train legs is because I have a torn meniscus in my knee and therefore spare my legs because I need surgery soon.Diet
| Morning | Clear Whey Isolate |
| Mid-Morning | Rice Pudding with Whey |
| Lunch | Chicken breast fillet with rice |
| Evening | Natural yogurt with flavor drops |
| Snack | Flexible 200-300kcal |
Training Experience
I personally started strength sports at age 16, however with many training breaks. First I went down from 16 years old with a BF of 45% from 88kg to 65kg and then into the build up to 78kg and then a cut to 74kg and then always had some interruptions due to work and injuries so that I always had sporadic 7 months of training then 5-6 months of breaks etc. Now I come back from a 7-month break from sports.Progression – Week 6 (Current)
I am now in week 6 since the first exogenous testosterone injection and have done another blood test to see how my body reacts to it.Based on my blood test, you can see that my HDL/LDL value is extremely bad, which is due to the fact that I did not do any cardio training to stabilize these values. To do this now, I additionally do cardio, supplement more omega 3, and continue my diet for body fat reduction.
You can also see that my estradiol E2 value is extremely elevated, which is due to my high body fat percentage. As a countermeasure, I have decided to take an aromatase inhibitor. I personally decided on anastrozole 0.5mg daily (ED) and will therefore do another quick lab test for my estradiol in 7 days to see how quickly it drops and then in 14 days when steady state is reached, do another lab test for my estradiol to adjust the dosage accordingly.
Important: With E2 = 162 pg/ml, monitoring is particularly critical because my body fat is simultaneously decreasing (through diet + clen) and this also lowers aromatase activity. This means my E2 could drop faster than normal and therefore I should already check after 7 days to not overshoot.
For you as a nice to know: please consider that there are anastrozole non-responders and if you should be one of them, you should switch to other aromatase inhibitors such as exemestane or letrozole etc.
Countermeasures (from Week 6)
E2 Management:
- Anastrozole 0.5mg ED starting now
- Test after 14 days (Steady State)
- Target range: 30-50 pg/ml
Lipid Management:
- Cardio 3-4x per week (30 min moderate intensity)
- Omega-3 supplementation: 3-4g daily
- Diet: Further caloric deficit for BF reduction
- Goal: HDL >50, LDL <100 within 8-12 weeks
I wrote the complete text myself, but I had it translated into English by an AI since I'm not that good at writing in this language as I'm from Germany. I created the tables myself for a structured overview. I hope I don't get hate for this since I just want to help. Thank you all!